What is Proning and How Does it Help with COVID-19 Patients?

Dr.Poonam Sharma
May 25, 2021
Dr.Poonam Sharma
May 25, 2021
SARS-CoV-2 virus causes pneumonia that is identified through fever, dyspnea, acute respiratory symptoms and named COVID-19. This disease exacerbates in a number of patients and causes pulmonary edema, multi-organ failure, and acute respiratory distress syndrome (ARDS).
Prevalence of ARDS among COVID-19 patients has been reported to be up to 17%. Among the introduced treatment methods for management of ARDS patients, prone position can be used as an adjuvant therapy for improving ventilation in these patients.
Lying face down is known as proning, it is a medically accepted position to improve oxygenation. It is especially beneficial in compromised COVID-19 patients with or without ventilator needs. If a patient’s oxygen levels drop below 94% (when measured at home on an oximeter), the patient can lie on their tummy; this position improves ventilation and enables comfortable breathing
The position allows for better expansion of the dorsal (back) lung regions, improved body movement and enhanced removal of secretions which may ultimately lead to advances in oxygenation (breathing).
Prone positioning has been shown to improve oxygenation for decades. However, proning in awake, non-intubated patients gained acceptance in the last few months since the onset of coronavirus (COVID-19) pandemic. To overcome the shortage of ventilators, to decrease the overwhelming burden on intensive care beds in the pandemic era, and also as invasive ventilation was associated with poor outcomes, proning of awake, spontaneously breathing patients gathered momentum.
Being an intervention with minimal risk and requiring minimum assistance, it is now a globally accepted therapy to improve oxygenation in acute hypoxemic respiratory failure in COVID-19 patients. We thus reviewed the literature of awake proning in non-intubated patients and described a safe protocol to practice the same.
Physical position affects the distribution and volume of air in the lungs, and can have direct effects on the expansion of the lungs to permit the exchange of oxygen & carbon dioxide in the blood.
In the last few years, prone positioning has been used increasingly in the treatment of patients with Acute Respiratory Distress Syndrome (ARDS) and this is now considered a simple and safe method to improve oxygenation. It is a medically accepted process that involves turning a patient with precise, safe motions, from their back onto their abdomen so that the individual is lying face down to improve breathing.
Proning is required only when the patient experiences difficulty in breathing and the SpO2 decreases below 94%. Regular monitoring of SpO2, along with other signs like temperature, blood pressure, and blood sugar, is important during home isolation. Missing out on Hypoxia (compromised oxygen circulation) may lead to worsening of complications.
Therefore, advice must be taken from the doctor on ways to effectively practice proning at home.
In the supine position, the lungs are compressed by the heart and abdominal organs. Gas exchange, the process of trading carbon dioxide for oxygen, is reduced in areas of collapsed lungs, resulting in low oxygen levels. In the prone position, lung compression is less improving lung function.
The body has mechanisms to adjust blood flow to different portions of the lung. Prone positioning redistributes blood and air flow more evenly, reducing this imbalance and improving gas exchange.
With improved lung function in the prone position, less support from the ventilator is needed to achieve adequate oxygen levels. This may reduce risk of ventilator-induced lung injury, which occurs from overinflation and excess stretching of certain portions of the lung.
Prone positioning may improve heart function in some patients. In the prone position, blood returns to the chambers on the right side of the heart increases and constriction of the blood vessels of the lung decreases. This may help the heart pump better, resulting in improved oxygen delivery to the body.
Because the mouth and nose are facing down in the prone position, secretions produced by the disease process in the lung may drain better.
Patients experiencing mild respiratory distress who do not need a ventilator, or those who could progress to severe respiratory distress, show improved oxygenation from proning.
There is not enough evidence at this time to prove that proning alleviates patients needing ventilators. “What we can see, though, is that oxygenation is temporarily improved. This is why proning has become part of the plan of care during the COVID-19 pandemic.”
Some investigators have reported the application of prone positioning in spontaneously breathing, non-intubated patients treated with standard oxygen therapy, continuous positive airway pressure (CPAP), or non-invasive ventilation.In this setting, prone positioning seems to improve oxygenation and might decrease respiratory effort, which could be particularly beneficial in patients at increased risk of self-induced lung injury.
Therefore, this position might postpone or avoid tracheal intubation and its inherent risks (both linked to the procedure itself and to subsequent superinfections). A decrease in the need for intubation, and subsequent admission to ICU, might also prove beneficial in resource-limited scenarios. At the same time, this procedure could carry some risks associated with the change of position (eg, vomiting, thromboembolism) or delayed intubation.
Proning techniques are done in hospitalised intubated patients. Self proning or awake proning is being suggested in patients with COVID-19 recently to improve oxygenation.
Note: Self-proning is a good way to boost oxygen levels at critical times when securing medical help may not be possible or manage symptoms at home. However, remember, it is only one of the ways that guarantee temporary relief and not a proper alternative for hospitalized care or oxygen support.
Not all patients who test positive for coronavirus and put under home care need the help of proning. However, the ones who may be facing oxygen deprivation, or waiting for medical help, simply lying down on your stomach could be a great help.
Proning should be especially tried when oxygen levels start to drop below 94% and continue to fluctuate through the day if external support is hard to find.
To sleep in the prone position, one needs to have plenty of pillows and keep changing positions on a half-hourly basis.
All patients with SpO2 <94% and RR >22/minute should be advised early awake proning.
Though the benefits of awake proning in mild COVID-19 disease have not been studied, the strategy is still encouraged. Patients on oxygen supplementation via nasal prongs, oxygen mask, NRBM, HFNC, and NIV, can be safely self-proned, as per their tolerance and comfort.
One may prone for up to 16 hours a day, in multiple cycles, suitable to a patient’s comfort and ability. Pillows may be adjusted slightly to alter pressure areas and for comfort. Keep a track of any pressure sores or injuries, especially around the bony prominence. If this is done with a help of a caregiver:

Place one pillow below the neck

Place one or two pillows below the chest through the upper thighs

Place two pillows below the shins
For self-proning:
According to The National Disaster Management Authority (NDMA) the correct way to achieve the benefits of proning.
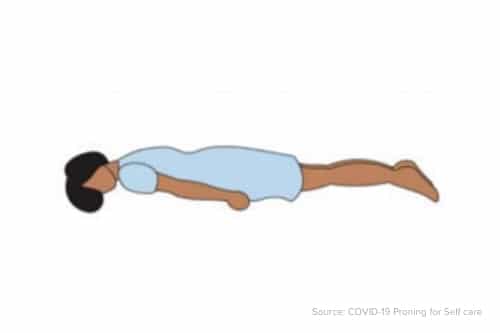
30 minutes to 2 hours: Lying on your belly

30 minutes to 2 hours: Lying on your right side
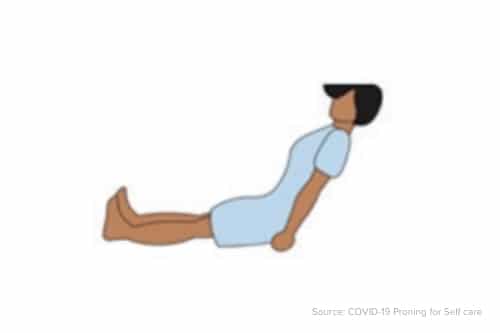
30 minutes to 2 hours: Sitting up
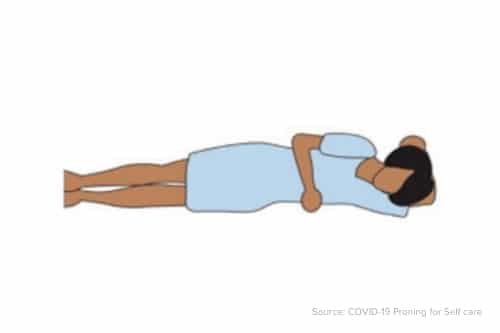
30 minutes to 2 hours: Lying on your left side
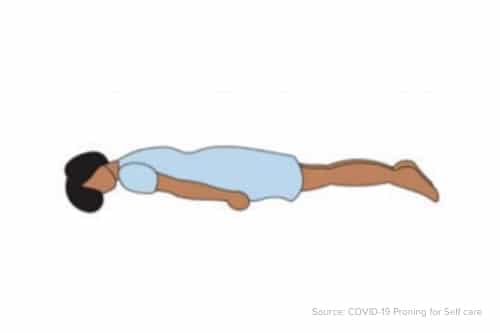
Then go back to position 1: Lying on your belly
Proning is very beneficial for COVID-19 patients with breathing complications, especially during home isolation.
Note: Always first please speak to your doctor before trying the self proning technique.
There is no specific recommendation for how long a patient should be self-proned. We suggest that awake, self-proning should be continued till the patient is comfortable, or has recovered and maintaining oxygen saturation >96% on room air, and has no respiratory distress/desaturation on exertion.
In a sick patient, proning should be interrupted if there is evidence of increased work of breathing, use of accessory muscles of respiration, failure of improvement in oxygenation with proning/further desaturation, or hemodynamic instability/arrhythmias.
An improvement in oxygen saturation on awake proning should not be an assurance of the improvement in the disease condition. Vigilance should be kept for signs of respiratory distress or increased work of breathing, which are an indication to interrupt awake proning and the need for invasive ventilation. The decision to intubate and invasively ventilate should be based on clinical assessment of work of breathing and other clinical criteria. Delaying intubation, just due to improvement in oxygenation, can lead to catastrophic outcomes.
In conclusion, awake, non-intubated patients appear to greatly benefit from self‐proning and alternating positioning, with many being able to independently change positions without disrupting the flow of oxygen.
Sources:
A. Proning is thought to distribute oxygen more evenly throughout the lungs and improve overall oxygenation. It’s commonly used for patients who are sedated and already on mechanical ventilation. However, it’s not standard practice for awake patients who are in respiratory distress but breathing on their own. One case report at the time briefly mentioned proning might help those with COVID-19, so given the circumstances it was worth a try.
A. In the prone position, it’s possible to aspirate food or fluid into the lungs, which is why our study excluded patients with altered mental state and those who couldn’t turn themselves over. Also, patients need to be closely monitored. But there’s a huge potential reward: sparing patients an even riskier procedure intubation and its complications.
A. It improves ventilation and makes breathing easier. It is especially helpful if your SPO2 goes below 94.

